
Today 29th August!
1) what is epidemiology of maxillary sinus carcinoma?
2)how often optiuc nerve is involved in maxillary sinus carcinoma and in which stage/
3) what is the percentage of Laryngeal carcer metastising to lung?
4)is there any incidence of laryngeal cancer metastising to abdominal muscle?
5) comparison of larynx cancer in the United states and India?
60How much healthcare cost laryngeal cancer add to the united states?
7) What is our responsiblity as publ;ic health specialist in light of Ca larynx?
8)Celebrities died or dying or diagnosed as larynx ca
9) Blood supply and lymphatic supply of larynx?
10) Important medical litigations in larynx cancer (online search)
brain metastases from Parotid…
Multiple brain metastases from adenoid cystic carcinoma of the parotid gland. Case report and review of the literature.
Source
Neurosurgery Clinic, Saitama Cancer Center, Ina, Japan.
Abstract
BACKGROUND:
Adenoid cystic carcinoma is a slow-growing malignant tumor occurring in the head and neck. Intracranial involvement usually results from direct skull invasion from adjacent primary sites. To our knowledge, this is the first reported case of multiple brain parenchymal metastases manifesting with hemorrhage.
CASE DESCRIPTION:
A 60-year-old male experienced sudden onset of hemiparesis caused by an intracerebral hematoma in a brain metastasis from adenoid cystic carcinoma. The primary parotid tumor was treated 15 months before the appearance of the brain metastases. The hemorrhagic metastasis was resected, and cranial irradiation was performed. The brain metastasis had increased cellular atypism compared with the primary tumor. The patient remained well and free of neurologic dysfunctions until 5 months after the radiotherapy was completed; he died of systemically advanced disease 8 months after the craniotomy.
CONCLUSION:
Hematogeneous brain metastases of adenoid cystic carcinoma are quite rare and cannot be distinguished from those of other cancers radiologically. We assume that the intratumoral hemorrhage is related to the tendency of the tumor to spread around the vessels. Although radiation therapy is not curative, it is beneficial in controlling tumor regrowth.
The same case I just came across. This article has been really handy!!
President Obama announces support for closing the self-referral loophole for radiation therapy services
President Obama’s budget for 2014, released today, includes a proposal to exclude radiation therapy services from the in-office ancillary services exception of the self-referral law. The budget estimates that excluding radiation therapy, as well as advanced imaging and physical therapy services, from the exception will save Medicare more than $6 billion over 10 years. Closing this loophole has been our top legislative priority for many years. ASTRO sent numerous letters encouraging the President to take this position, and our staff recently met with senior White House officials to urge them to close the loophole for radiation therapy services. The budget states:
Exclude Certain Services from the In-Office Ancillary Services Exception: The in-office ancillary services exception was intended to allow physicians to self refer quick turnaround services. While there are many appropriate uses for this exception, certain services, such as advanced imaging and outpatient therapy, are rarely performed on the same day as the related physician office visit. Additionally, evidence suggests that this exception may have resulted in overutilization and rapid growth of certain services. Effective calendar year 2015, this proposal would seek to encourage more appropriate use of select services by excluding radiation therapy, therapy services and advanced imaging from the in-office ancillary services exception to the prohibition against physician self-referrals (Stark law), except in cases where a practice meets certain accountability standards, as defined by the Secretary. [$6.1 billion in savings over 10 years]
While the budget is a proposal and will not likely be enacted into law given the partisan differences on key budget issues, inclusion in the President’s proposal is a huge boost to our advocacy efforts. It will serve as the starting point for budget negotiations and potentially Medicare reform. ASTRO will continue working with Congress to achieve our ultimate goal of permanently closing the self-referral loophole. We will provide more analysis as further details emerge. Click
RTOG Radiation toxicity grading!
Skin: Grade 1: dull erythema, decreased sweating. Grade 2: moderate edema, bright erythema, pitting edema Grade 4″ Ulceration, hemorrhage and necrosis.
Mucous membrane: Grade 1:mild pain at injection site Grade2:inflammatory serosanguinous discharge Grade 3:confluent fibrinous mucositis Grade 4: Unceration, hemarhhage or necrosis.
Eye: Grade 1: mild conjuctivits, grade2: moderate conjuctivits grade3: sevre keratitis ,acute glaucoma Grade4: loss opf vision.
Medulloblastoma!
As we have the discussion over medullobastome to day, I thought to revise it briefly.
The commonest malignancyin children, accounting for 10-20% of primary Neuro neoplasm and approximately 40% of all posterior fossa tumors.
From the diagram, we can see the malignancy from cerebellum(Cerebellar vermis). If the same growth occurs in other part of CNS, it is termed as primitive neuroectodermal tumor. Though 50% of medulloblastoma patients can be treated with surgery and chemotherapy, endocrine and neural functions are compromised. 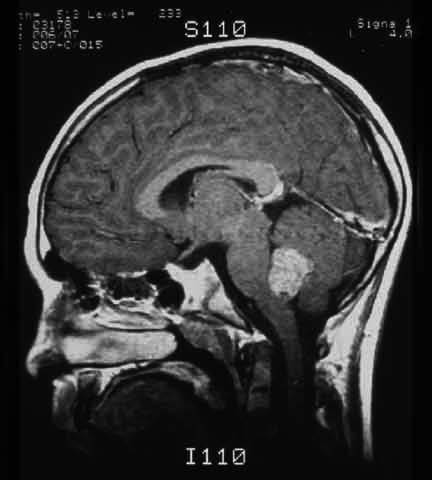
ncogenes ERBB2 andMYCC are associated with worse outcome. Of all pediatric neoplasms, medulloblastoma has highest propensity to spread extra neural sites, specially bone and bone marrow. But it is not more than 4 percent.
Hydrocephalus: reason is obstruction of CSF through 4th ventricle.
Epidemiology:
No racial predisposition is noted. Data shows patients aged 0-14 years in the United States have an incidence rate per million population of 5.7 in whites and 5 in blacks.
US incidence per 1 million population for patients aged 0-14 years is 6.1 for boys and 4.5 for girls.
Peak age of incidence is 3-5 years. Approximately 80% of patients are diagnosed in the first 15 years of life. WHile I was doing my internship project with Einstein, our sample didn’t have pediatric age group
Symptoms:
1)Increased intracranial pressure: Headache, Vomitting and lethargy
2)Cerebellar functions compromised: ATaxia worsens
3)Brain Stem Deficit: Most of the functions of cranial nerves are affected: for example 7th and 8th nerve: facial weakness, tinnitus, hearing loss, head tilt, and stiff neck.
Hereditary Association: isochromosome 17q [i(17q)].
Differential Diagnosis: Epindymoma, Astrocytome, Aseeptic Meningtis, Bacterial Meningits.
In a report by the International Society of Pediatric Oncology, children with average-risk medulloblastoma randomly received either the standard 36 Gy or a reduced dose of 24 Gy to the neuraxis (Tait et al). However, the role of radiation therapy in the patients younger than 3 years remain controversial. What is survival rate?
(Source:emedicine)